
Page 153 - 20211214_OHKF_Health_Finance_Research_Report_E (1)
P. 153
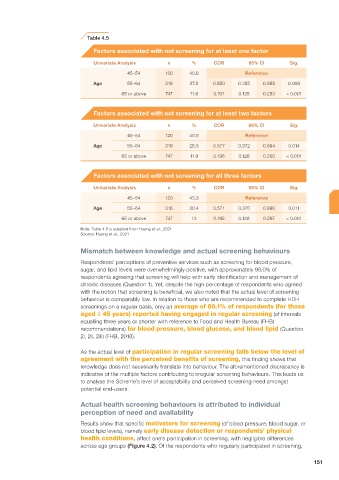
Table 4.5
Factors associated with not screening for at least one factor
Univariate Analysis n % COR 95% CI Sig.
45–54 120 40.8 Reference
Age 55–64 316 27.5 0.550 0.355 0.855 0.008
65 or above 747 11.6 0.191 0.125 0.293 < 0.001
Factors associated with not screening for at least two factors
Univariate Analysis n % COR 95% CI Sig.
45–54 120 40.8 Reference
Age 55–64 316 28.5 0.577 0.372 0.894 0.014
65 or above 747 11.9 0.196 0.128 0.300 < 0.001
Factors associated with not screening for all three factors
Univariate Analysis n % COR 95% CI Sig.
45–54 120 43.3 Reference
Age 55–64 316 30.4 0.571 0.370 0.880 0.011
65 or above 747 13 0.195 0.128 0.297 < 0.001
Note: Table 4.5 is adapted from Huang et al., 2021
Source: Huang et al., 2021
Mismatch between knowledge and actual screening behaviours
Respondents’ perceptions of preventive services such as screening for blood pressure,
sugar, and lipid levels were overwhelmingly positive, with approximately 98.0% of
respondents agreeing that screening will help with early identification and management of
chronic diseases (Question 1). Yet, despite the high percentage of respondents who agreed
with the notion that screening is beneficial, we also noted that the actual level of screening
behaviour is comparably low. In relation to those who are recommended to complete HDH
screenings on a regular basis, only an average of 80.1% of respondents (for those
aged ≥ 45 years) reported having engaged in regular screening (of intervals
equalling three years or shorter with reference to Food and Health Bureau (FHB)
recommendations) for blood pressure, blood glucose, and blood lipid (Question
2i, 2ii, 2iii) (FHB, 2018).
As the actual level of participation in regular screening falls below the level of
agreement with the perceived benefits of screening, this finding shows that
knowledge does not necessarily translate into behaviour. The aforementioned discrepancy is
indicative of the multiple factors contributing to irregular screening behaviours. This leads us
to analyse the Scheme’s level of acceptability and perceived screening need amongst
potential end-users.
Actual health screening behaviours is attributed to individual
perception of need and availability
Results show that specific motivators for screening (of blood pressure, blood sugar, or
blood lipid levels), namely early disease detection or respondents’ physical
health conditions, affect one’s participation in screening, with negligible differences
across age groups (Figure 4.2). Of the respondents who regularly participated in screening,
151