
Page 49 - 20211214_OHKF_Health_Finance_Research_Report_E (1)
P. 49
inputs to providers, often in the form of salaries or payments, who then provide services to
the beneficiaries defined; patients may also be required to provide some additional
payments, i.e. co-payments, to providers in order to receive care. Under a capitation
payment structure, providers receive a fixed amount of financial reimbursement within a
given time span to care for a defined population. This payment system is likely to incentivise
under-provision of care in order to maximise profits and requires closer monitoring and
analysis for necessary health services and procedures to ensure they are provided.
A fee-for-service payment structure offers a fixed payment for each service
provided, facilitates access to care but also incentivises over-provision and unnecessary
care. A pay-for-performance (PFP) payment structure attempts to link a set
payment for defined health targets or outcomes. This format is also named performance-
based financing or results-based financing. PFP may encourage more efficient use of
resources but may over- or under-incentivise care based on the health target of each patient.
Demand-side financing operates under the principle that if individuals were not limited by
financial restrictions, they would seek out healthcare services. As such, demand-side
financing formats feature a payment organisation, such as a voucher agency, providing the
entitlement to a subsidy to individuals, who will then seek care from providers, using the
voucher as a form of payment (The World Bank, 2004; WHO, 2010a). Vouchers are meant to
reduce the financial hardship incurred when seeking care by enhancing the purchasing
power of patients. The use and distribution of vouchers can spur demand for specified
under-utilised services, especially by specific target populations.
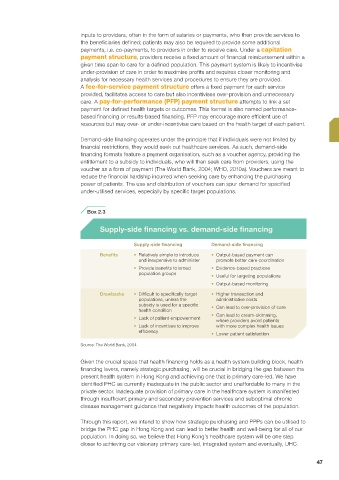
Box 2.3
Supply-side financing vs. demand-side financing
Supply-side financing Demand-side financing
Benefits • Relatively simple to introduce • Output-based payment can
and inexpensive to administer promote better care coordination
• Provide benefits to broad • Evidence-based practices
population groups
• Useful for targeting populations
• Output-based monitoring
Drawbacks • Difficult to specifically target • Higher transaction and
populations, unless the administrative costs
subsidy is used for a specific • Can lead to over-provision of care
health condition
• Can lead to cream-skimming,
• Lack of patient empowerment
where providers avoid patients
• Lack of incentives to improve with more complex health issues
efficiency • Lower patient satisfaction
Source: The World Bank, 2004
Given the crucial space that health financing holds as a health system building block, health
financing levers, namely strategic purchasing, will be crucial in bridging the gap between the
present health system in Hong Kong and achieving one that is primary care-led. We have
identified PHC as currently inadequate in the public sector and unaffordable to many in the
private sector. Inadequate provision of primary care in the healthcare system is manifested
through insufficient primary and secondary prevention services and suboptimal chronic
disease management guidance that negatively impacts health outcomes of the population.
Through this report, we intend to show how strategic purchasing and PPPs can be utilised to
bridge the PHC gap in Hong Kong and can lead to better health and well-being for all of our
population. In doing so, we believe that Hong Kong’s healthcare system will be one step
closer to achieving our visionary primary care-led, integrated system and eventually, UHC.
47