
Page 22 - 20211214_OHKF_Health_Finance_Research_Report_E (1)
P. 22
who lack financial means do not receive needed health services and may have to forgo care
(Wong et al., 2018). With regards to primary care access, those who were income-poor in
Hong Kong were reported as less likely to access a primary care provider and visit private
primary care doctors (Chung et al., 2019).
Table 1.1
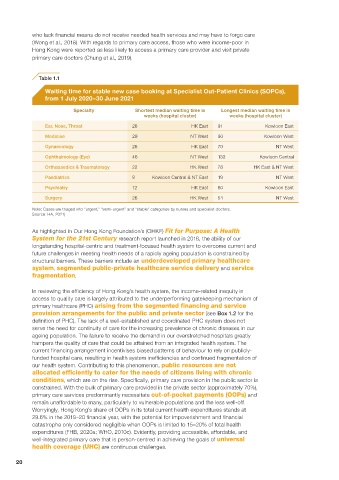
Waiting time for stable new case booking at Specialist Out-Patient Clinics (SOPCs),
from 1 July 2020–30 June 2021
Specialty Shortest median waiting time in Longest median waiting time in
weeks (hospital cluster) weeks (hospital cluster)
Ear, Nose, Throat 26 HK East 91 Kowloon East
Medicine 29 NT West 90 Kowloon West
Gynaecology 26 HK East 70 NT West
Ophthalmology (Eye) 46 NT West 133 Kowloon Central
Orthopaedics & Traumatology 22 HK West 78 HK East & NT West
Paediatrics 8 Kowloon Central & NT East 19 NT West
Psychiatry 12 HK East 60 Kowloon East
Surgery 26 HK West 54 NT West
Note: Cases are triaged into “urgent,” “semi-urgent” and “stable” categories by nurses and specialist doctors.
Source: HA, 2021j
As highlighted in Our Hong Kong Foundation’s (OHKF) Fit for Purpose: A Health
System for the 21st Century research report launched in 2018, the ability of our
longstanding hospital-centric and treatment-focused health system to overcome current and
future challenges in meeting health needs of a rapidly ageing population is constrained by
structural barriers. These barriers include an underdeveloped primary healthcare
system, segmented public-private healthcare service delivery and service
fragmentation.
In reviewing the efficiency of Hong Kong’s health system, the income-related inequity in
access to quality care is largely attributed to the underperforming gatekeeping mechanism of
primary healthcare (PHC) arising from the segmented financing and service
provision arrangements for the public and private sector (see Box 1.2 for the
definition of PHC). The lack of a well-established and coordinated PHC system does not
serve the need for continuity of care for the increasing prevalence of chronic diseases in our
ageing population. The failure to receive the demand in our overstretched hospitals greatly
hampers the quality of care that could be attained from an integrated health system. The
current financing arrangement incentivises biased patterns of behaviour to rely on publicly-
funded hospital care, resulting in health system inefficiencies and continued fragmentation of
our health system. Contributing to this phenomenon, public resources are not
allocated efficiently to cater for the needs of citizens living with chronic
conditions, which are on the rise. Specifically, primary care provision in the public sector is
constrained. With the bulk of primary care provided in the private sector (approximately 70%),
primary care services predominantly necessitate out-of-pocket payments (OOPs) and
remain unaffordable to many, particularly to vulnerable populations and the less well-off.
Worryingly, Hong Kong’s share of OOPs in its total current health expenditures stands at
29.6% in the 2019–20 financial year, with the potential for impoverishment and financial
catastrophe only considered negligible when OOPs is limited to 15–20% of total health
expenditures (FHB, 2020a; WHO, 2010c). Evidently, providing accessible, affordable, and
well-integrated primary care that is person-centred in achieving the goals of universal
health coverage (UHC) are continuous challenges.
20