
Page 264 - 20211214_OHKF_Health_Finance_Research_Report_E (1)
P. 264
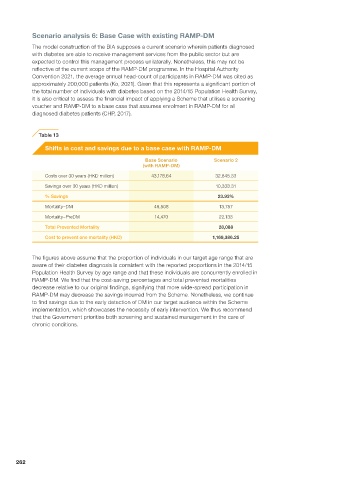
Scenario analysis 6: Base Case with existing RAMP-DM
The model construction of the BIA supposes a current scenario wherein patients diagnosed
with diabetes are able to receive management services from the public sector but are
expected to control this management process unilaterally. Nonetheless, this may not be
reflective of the current scope of the RAMP-DM programme. In the Hospital Authority
Convention 2021, the average annual head-count of participants in RAMP-DM was cited as
approximately 200,000 patients (Ko, 2021). Given that this represents a significant portion of
the total number of individuals with diabetes based on the 2014/15 Population Health Survey,
it is also critical to assess the financial impact of applying a Scheme that utilises a screening
voucher and RAMP-DM to a base case that assumes enrolment in RAMP-DM for all
diagnosed diabetes patients (CHP, 2017).
Table 13
Shifts in cost and savings due to a base case with RAMP-DM
Base Scenario Scenario 2
(with RAMP-DM)
Costs over 30 years (HKD million) 43,178.64 32,845.33
Savings over 30 years (HKD million) 10,333.31
% Savings 23.93%
Mortality–DM 49,508 13,757
Mortality–PreDM 14,470 22,133
Total Prevented Mortality 28,088
Cost to prevent one mortality (HKD) 1,169,386.25
The figures above assume that the proportion of individuals in our target age range that are
aware of their diabetes diagnosis is consistent with the reported proportions in the 2014/15
Population Health Survey by age range and that these individuals are concurrently enrolled in
RAMP-DM. We find that the cost-saving percentages and total prevented mortalities
decrease relative to our original findings, signifying that more wide-spread participation in
RAMP-DM may decrease the savings incurred from the Scheme. Nonetheless, we continue
to find savings due to the early detection of DM in our target audience within the Scheme
implementation, which showcases the necessity of early intervention. We thus recommend
that the Government prioritise both screening and sustained management in the care of
chronic conditions.
262