
Page 259 - 20211214_OHKF_Health_Finance_Research_Report_E (1)
P. 259
APPENDIX R: SCENARIO ANALYSIS RESULTS
Scenario analysis 1: Variation in remission rates
The model employs a remission variable of 7% to indicate rate of remission from diabetes
towards prediabetes after intervention–namely screening and participation in a risk
assessment and diabetes management programme (Ried‐Larsen et al., 2019). Nonetheless,
literature shows that remission is also associated with intensive lifestyle intervention and
bariatric surgery, which may not overlap with the treatment and management path that the
CDSVMS patients take (Gregg et al., 2012; Ried‐Larsen et al., 2019; Sjöström et al., 2009). To
assess the possible cost impact of different remission rates, we conducted scenario
analyses using remission rates of 2.0%, representing the remission rate for patients with
diabetes who only receive diabetes support and education in a different study (Gregg et al.,
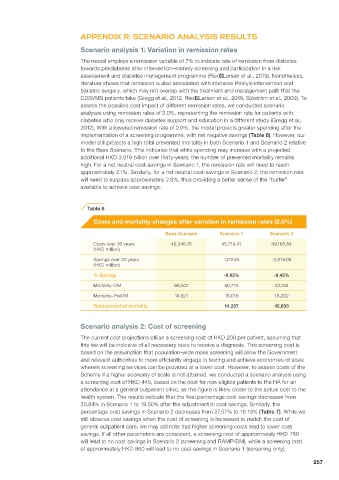
2012). With a lowered remission rate of 2.0%, the model projects greater spending after the
implementation of a screening programme, with net negative savings (Table 6). However, our
model still projects a high total prevented mortality in both Scenario 1 and Scenario 2 relative
to the Base Scenario. This indicates that while spending may increase with a projected
additional HKD 3.819 billion over thirty-years, the number of prevented mortality remains
high. For a net neutral cost-savings in Scenario 1, the remission rate will need to reach
approximately 2.1%. Similarly, for a net neutral cost-savings in Scenario 2, the remission rate
will need to surpass approximately 2.9%, thus providing a better sense of the “buffer”
available to achieve cost-savings.
Table 6
Costs and mortality changes after variation in remission rates (2.0%)
Base Scenario Scenario 1 Scenario 2
Costs over 30 years 45,346.76 45,719.41 49,165.84
(HKD million)
Savings over 30 years -372.65 -3,819.08
(HKD million)
% Savings -0.82% -8.42%
Mortality–DM 68,507 50,775 22,193
Mortality–PreDM 14,521 18,016 18,202
Total prevented mortality 14,237 42,633
Scenario analysis 2: Cost of screening
The current cost projections utilise a screening cost of HKD 200 per patient, assuming that
this fee will be inclusive of all necessary tests to receive a diagnosis. This screening cost is
based on the assumption that population-wide mass screening will allow the Government
and relevant authorities to more efficiently engage in testing and achieve economies of scale
wherein screening services can be provided at a lower cost. However, to assess costs of the
Scheme if a higher economy of scale is not attained, we conducted a scenario analysis using
a screening cost of HKD 445, based on the cost for non-eligible patients to the HA for an
attendance at a general outpatient clinic, as this figure is likely closer to the actual cost to the
health system. The results indicate that the final percentage cost savings decreases from
30.84% in Scenario 1 to 19.50% after the adjustment in cost savings. Similarly, the
percentage cost savings in Scenario 2 decreases from 27.57% to 16.19% (Table 7). While we
still observe cost savings when the cost of screening is increased to match the cost of
general outpatient care, we may still note that higher screening costs lead to lower cost
savings. If all other parameters are consistent, a screening cost of approximately HKD 780
will lead to no cost savings in Scenario 2 (screening and RAMP-DM), while a screening cost
of approximately HKD 860 will lead to no cost-savings in Scenario 1 (screening only).
257