
Page 185 - 20211214_OHKF_Health_Finance_Research_Report_E (1)
P. 185
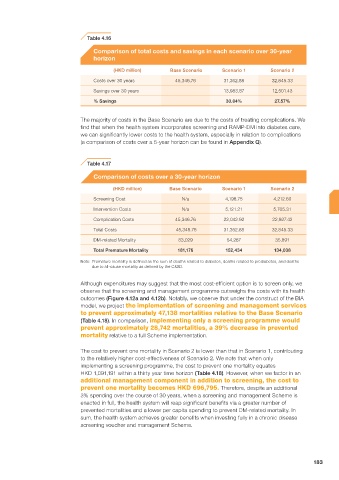
Table 4.16
Comparison of total costs and savings in each scenario over 30-year
horizon
(HKD million) Base Scenario Scenario 1 Scenario 2
Costs over 30 years 45,346.76 31,362.88 32,845.33
Savings over 30 years 13,983.87 12,501.43
% Savings 30.84% 27.57%
The majority of costs in the Base Scenario are due to the costs of treating complications. We
find that when the health system incorporates screening and RAMP-DM into diabetes care,
we can significantly lower costs to the health system, especially in relation to complications
(a comparison of costs over a 5-year horizon can be found in Appendix Q).
Table 4.17
Comparison of costs over a 30-year horizon
(HKD million) Base Scenario Scenario 1 Scenario 2
Screening Cost N/a 4,198.75 4,212.60
Intervention Costs N/a 5,121.21 5,705.31
Complication Costs 45,346.76 22,042.92 22,927.42
Total Costs 45,346.76 31,362.88 32,845.33
DM-related Mortality 83,029 54,287 35,891
Total Premature Mortality 181,176 152,434 134,038
Note: Premature mortality is defined as the sum of deaths related to diabetes, deaths related to prediabetes, and deaths
due to all-cause mortality as defined by the C&SD.
Although expenditures may suggest that the most cost-efficient option is to screen only, we
observe that the screening and management programme outweighs the costs with its health
outcomes (Figure 4.12a and 4.12b). Notably, we observe that under the construct of the BIA
model, we project the implementation of screening and management services
to prevent approximately 47,138 mortalities relative to the Base Scenario
(Table 4.18). In comparison, implementing only a screening programme would
prevent approximately 28,742 mortalities, a 39% decrease in prevented
mortality relative to a full Scheme implementation.
The cost to prevent one mortality in Scenario 2 is lower than that in Scenario 1, contributing
to the relatively higher cost-effectiveness of Scenario 2. We note that when only
implementing a screening programme, the cost to prevent one mortality equates
HKD 1,091,191 within a thirty year time horizon (Table 4.18). However, when we factor in an
additional management component in addition to screening, the cost to
prevent one mortality becomes HKD 696,795. Therefore, despite an additional
3% spending over the course of 30 years, when a screening and management Scheme is
enacted in full, the health system will reap significant benefits via a greater number of
prevented mortalities and a lower per capita spending to prevent DM-related mortality. In
sum, the health system achieves greater benefits when investing fully in a chronic disease
screening voucher and management Scheme.
183